1
Palpate the midsection for firmness or rigidity
People with HIV (PWHIV) have an increased risk in developing excess visceral abdominal fat.1
Excess visceral abdominal fat is the abnormal accumulation of visceral fat in the abdominal cavity and is present around internal organs.2
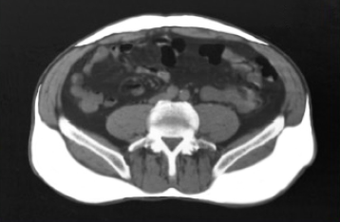
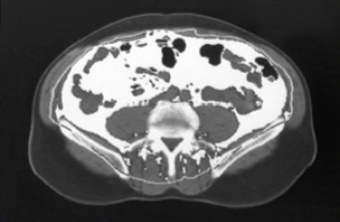
155 cm2
The pathogenesis of excess visceral abdominal fat in PWHIV appears to be multifactorial, including contributions from:2
Palpate the midsection for firmness or rigidity
Measure waist and hip circumferences
Calculate
waist‑to‑hip ratio†
Ensure both circumferences are entered with the same unit.
Waist circumference
≥37.4 in (95 cm)
Waist-to-hip ratio ≥0.94
Waist circumference
≥37 in (94 cm)
Waist-to-hip ratio ≥0.88
BMI and WC are independently associated with predicting excess visceral abdominal fat.4,5
BMI = body mass index; WC = waist circumference.
† Waist‑to‑hip ratio = waist circumference/hip circumference.
‡ Reference values are based on inclusion criteria in clinical trials.
References:
EGRIFTA SV® is indicated for the reduction of excess abdominal fat in people with HIV and lipodystrophy.
Do not use EGRIFTA SV® if patient:
The most commonly reported adverse reactions include injection site reactions, arthralgia, pain in extremity, myalgia, and peripheral edema.
For more information about EGRIFTA SV®, contact ![]() toll‑free at 1‑833‑23THERA (1‑833‑238-4372).To report suspected adverse reactions, contact
toll‑free at 1‑833‑23THERA (1‑833‑238-4372).To report suspected adverse reactions, contact ![]() at 1‑833‑23THERA (1‑833‑238-4372) or FDA at 1‑800‑FDA-1088 or www.fda.gov/medwatch.
at 1‑833‑23THERA (1‑833‑238-4372) or FDA at 1‑800‑FDA-1088 or www.fda.gov/medwatch.
Please see full Prescribing Information for EGRIFTA SV®.